File: <lymedisease.htm> <Medical
Index> <General Index> Site Description
Glossary <Navigate
to Home>
|
LYME DISEASE (Contact) Please CLICK on image
& underlined links for details:
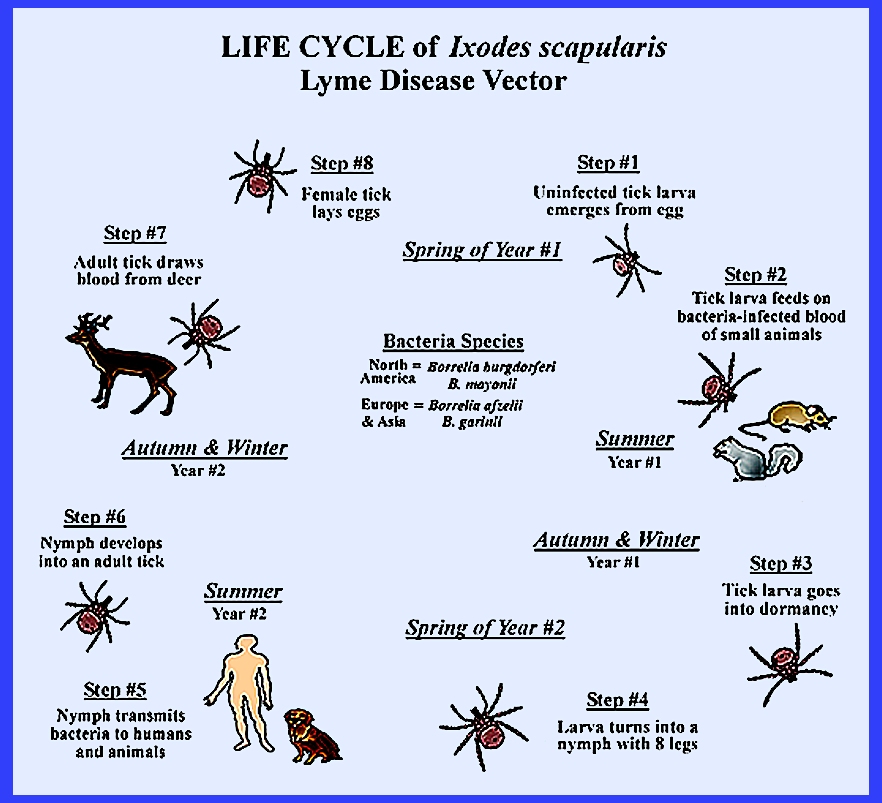
The disease is
an infection that is caused by bacteria of the genus Borrelia. Symptoms are an expanding area of redness that begins at the site
of a tick bite about 5-7 days after the attack. A rash develops that is neither prickly nor painful. About 25-50 percent of infected people do
not develop the rash. Other early
symptoms include fever and headache.
If untreated symptoms may extend to joint pain, severe headache, neck
stiffness, heart palpitations, etc.
Much later (months to years) repeated episodes of joint pain and
swelling may occur. Some patients
also develop shooting pains or tingling in their arms and legs. Even with treatment about 10-20 percent of
people develop joint pains, memory problems and weariness for at least 6
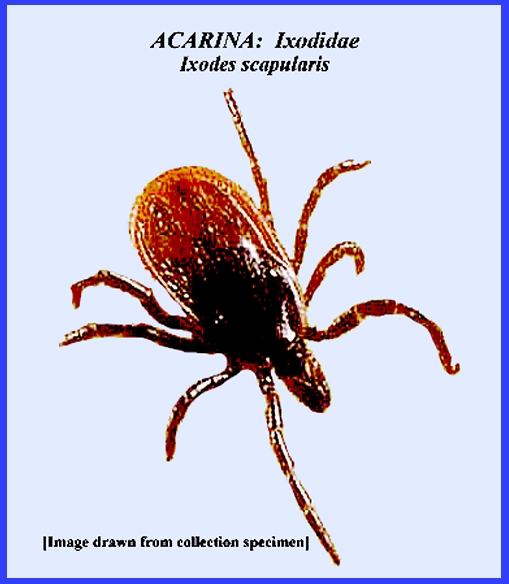
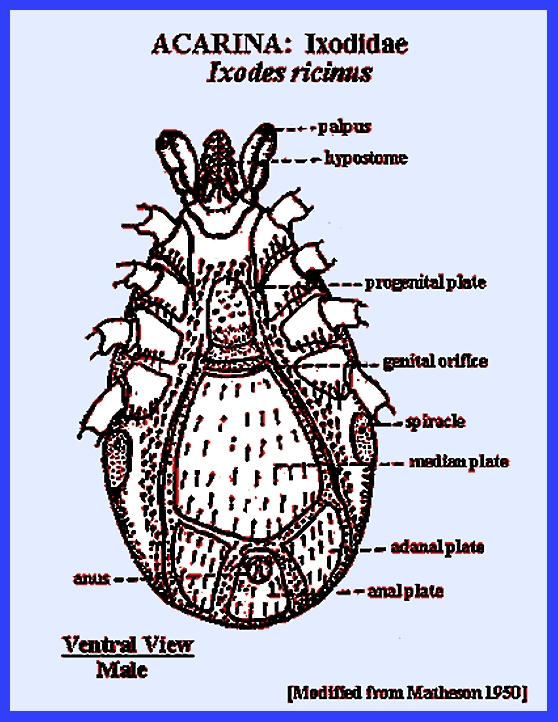
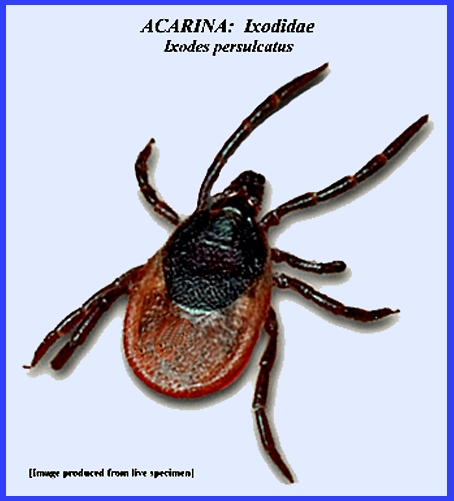
months. The disease is
transmitted to humans by the bite of bacteria-infected ticks of the genus Ixodes: Ixodes ricinus
in Europe, I. persulcatus in
Eurasia, I. scapularis in eastern United States and I. pacificus in
western states. Typically the tick
must be attached for 36-48 hours before the bacteria can spread. In North America, Borrelia burgdorferi and Borellia mayonii are the cause. In Europe and Asia the bacteria Borrelia afzelii and Borrelia garinii are also causes of the disease. The disease does not seem to be
transmitted among people, by other animals or through food. Diagnosis is based on a combination of
symptoms, history of tick exposure and by testing for specific antibodies in
the blood. However, blood tests are frequently negative in the early stages
of the disease. Testing of the ticks
themselves is not only impractical but also not reliable. Prevention
includes avoiding tick bites by wearing protective clothing or using
repellants such as DEET. Certain
pesticides may also be effective.
Ticks can be removed using tweezers.
If the removed tick was full of blood a single dose of doxycycline may
prevent infection. If an infection
develops there are a number of antibiotics available, including doxycycline,
amoxicillin and cefuroxime.
Treatments regularly require 2-3 weeks. Some patients develop a fever and muscle and joint pains from
treatment that may last a few days.
For persistent symptoms long-term antibiotic therapy has little
effect. = = = = = = = = = = = = = = = = = = = = Key References: <medvet.ref.htm> <Hexapoda> Camicas, J. L., J. . Hervy, F. Adam & P.
C. Morel. 1998. The ticks of the world (Acarida,
Ixodida): Nomenclature, Described Stages, Hosts, Distribution. Paris: Editions de l'ORSTOM. Dumler, J. S. & D.
H. Walker. 2005. Rocky mountain spotted fever: changing
ecology and persisting virulence. New
England J. of Med. 353: 551-53. Gammons, M. & G.
Salam. 2002. Tick removal. Amer. Fam. Physician 66:
643-45. Gothe, R., K. Kunze
& H. Hoogstraal. 1979. The mechanisms of pathogenicity in the
tick paralyses. J. Med. Ent. 16: 357-69. Gray, J. S., O. Kahl, R.
S. Lane & G. Stanek. 2002. Lyme Borreliosis: Biology, Epidemiology
& Control. CABI, Wallingford, England Hoogstraal, H. 1966.
Ticks in relation to human diseases caused by viruses. Ann. Rev. Ent. 11: 261-308. Hoogstraal, H. 1967.
Ticks in relation to human diseases caused by Rickettsia species. Ann. Rev. Ent. 12: 377-420. Lane, R. S., J. Piesman
& W. Burgdorfer. 1991. Lyme borreliosis: relation of its causative
agent to its vectors and hosts in North America and Europe. Ann. Rev. Ent.
36: 587-609. Matheson, R. 1950. Medical Entomology. Comstock Publ. Co, Inc. 610 p. Service, M. 2008.
Medical Entomology For Students.
Cambridge Univ. Press. 289 p Needham, G. R. & P.
D. Teel. 1991. Off-host physiological ecology of ixodid
ticks. Ann. Rev. Ent. 36: 313-52. Parola, P. & D. Raoult. 2001. Tick-borne typhuses.
IN: The Encyclopedia of
arthropod-transmitted Infections of Man and Domesticated Animals. ed. M. W.
Service, Wallingford: CABI: pp.
516-24. Sonenshine, D. E.,
R. S. Lane & W. L. Nicholson. 2002. Ticks (Ixodida).
IN: Medical & Veterinary
Entomology, ed. G. Mullen & L. Durden, Ambsterdam Acad.
Press. pp 517-58. Sonenshine, D. E. &
T. N. Mather (eds.) 1994. Ecological Dynamics of Tick-Borne
Zoonoses. Oxford Univ. Press, New
York. Steer, A., J. Coburn
& L. Glickstein. 2005. Lyme borreliosis. IN:
Tick-Borne Diseases of Humans, ed. J. L. Goodman, D. T. Dennis & D.
E. Sonenshine. Washington, DC: ASM Press. |
{kind=link}
{kind=link}
{kind=link}
{kind=link}